There are some choices that individuals have in relation to how their confidential patient information is used beyond their individual care. It’s quite a complex picture across the UK and will depend on where in the UK you receive care. This is because health is a devolved policy matter, which means each nation has its own rules, processes and data systems.
UPD has produced this guide so that individuals have as much information available to them as possible to make informed choices where there is the ability to do so. These choices are largely to remain opted-in by default, or opt-out. UPD does not recommend any particular choices.
The information below is split up into:
-
The picture across the UK (if you receive care in England, then some English policy will apply to you even if you live elsewhere)
-
Further information on opt-outs in England, covering the history, considering your choices and UPD’s analysis
-
Frequently asked questions
What is confidential patient information?
Confidential patient information identifies you and says something about your health, care or treatment. You would expect this information to be kept private and held securely. Information that only identifies you, like your name, and address, is not normally considered confidential patient information for the purposes of the national data opt-out, but it is personal data, and may still be used, e.g. to contact you about your care.
The Picture Across the UK
Northern Ireland:
There is not currently an opt-out policy in place in Northern Ireland. However, a regional opt-out is being introduced as part of the implementation of regulations following the Health and Social Care (Control of Data Processing) Act (Northern Ireland) 2016. This will enable people to opt out of having their confidential patient information used for reasons beyond direct care, where exemptions aren’t in place. The Northern Ireland Assembly expects providers of health and social care who process confidential and personal data to ensure they comply with the relevant legislation and the common law. Patients who do not wish their data to be shared outside of their GP practice in Northern Ireland should speak to their registered practice to discuss options and implications. Patients can also find further information via the Health and Social Care Privacy Advisory Committee.
Scotland:
There is no national policy in Scotland for opting-out of your health and care data being used for research purposes. Some specific research projects may make provision for opting-out of their research on a bespoke basis. Applications for research on health and care data in Scotland are scrutinised by the Public Benefit and Privacy Panel for Health and Social Care, whose role it is to ensure that applicants have thought through the public benefit and privacy implications of their proposal. The panel balances public benefit with potential risk to privacy and ensures that the public benefit will be furthered by the proposal, as well as demonstrating the social need for the processing of the data requested will result in tangible benefit for society. For more information on your health and social care data rights please see Annex B of Scotland’s Data Strategy for Health and Social Care.
Wales:
There is no opt-out policy in Wales. Welsh Government expects providers of health and care in Wales who process confidential and personal data to ensure they comply with the relevant legislation and common law. Health records of Welsh residents from health and care organisations in England are subject to the English opt-out policy. Patients who do not wish their data to be shared outside of their GP practice in Wales should speak to their registered practice to discuss options and implications and patients can also contact their local health board for further information.
England:
There is an opt-out policy in England. The main opt-out in place is the national data opt-out, which enables people to opt out of having their confidential patient information (across all health and adult social care services) used for research and planning, where exemptions aren’t in place (scroll down to “what the national data opt-out applies to” to see these). Planning and research include planning healthcare services and research conducted by academia, charities, and the private sector. The opt-outs available in England are DHSC policy, it is not a legal requirement to offer a national data opt out.
There is also a GP data opt-out (known as a Type 1 opt-out), which applies to GP data, in addition to the national data opt-out. This means that the data held in your GP medical record specifically is only shared outside of the GP practice for your individual care and agreed exemptions. Type 1 opt-outs may be discontinued in the future. If this happens then they may be turned into a national data opt-out, but this is awaiting further information.
Further Information on Opt-Out in England
This section is included because there is sometimes controversy relating to health data projects in England, more frequently than in Scotland, Wales and Northern Ireland, and more policies in place regarding opting out.
History of opt-out policy in England
The 2013 NHS Constitution for England stated that “you have the right to request that your confidential data is not used beyond your own care and treatment and to have your objections considered, and where your wishes cannot be followed, to be told the reasons including the legal basis”. This was because there were concerns about the safety of releasing individual-level health data, and about sharing data with external organisations.
An ability to opt-out at a national level national data opt-out was first introduced in January 2014 for patients in the English NHS in response to recommendations by Dame Fiona Caldicott (the then National Data Guardian) in her 2013 Information Governance Review and to meet the pledge in the NHS Constitution.
There was an additional Caldicott Review in 2016, focusing on data security, consent and opt-outs. This review highlighted that, whilst there was support for data being used for planning and research, there were also people that still wanted a choice, and the ways of opting out at the time were confusing. They tested and developed two models, one which allowed individuals to opt out of planning and research separately (two opt-outs), and one that kept planning and research together (one opt-out). Both approaches had pros and cons.
The model that was taken forwards kept planning and research together as a single opt-out, and was launched in 2018. The initial deadline for all health and care organisations to apply the opt-out was originally 2020, but this was extended to 2022 because of the Covid pandemic.
By now, every organisation in the NHS should respect the national data opt-out where it applies.
Statistics about opt outs in England
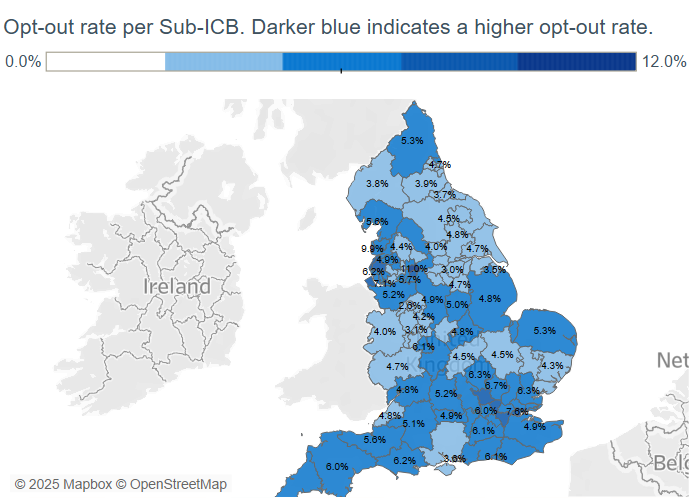
The level of opt out across England has been relatively stable for the last few years at around 5.6% of the population. Data on the levels of national data opt-outs in total and broken down by demographic groups is published by NHS England here.
We know that opt-out rates are not entirely consistent by demographic groups, and some groups are more likely to opt out than others. For instance, opt-out rates are slightly higher in the least deprived areas (6.2%) vs the most deprived (4.9%), and women are more likely to opt out than men (6.2% versus 4.9%). The opt-out rate is the highest in London (7.1%) and the lowest in North East and Yorkshire (4.3%).
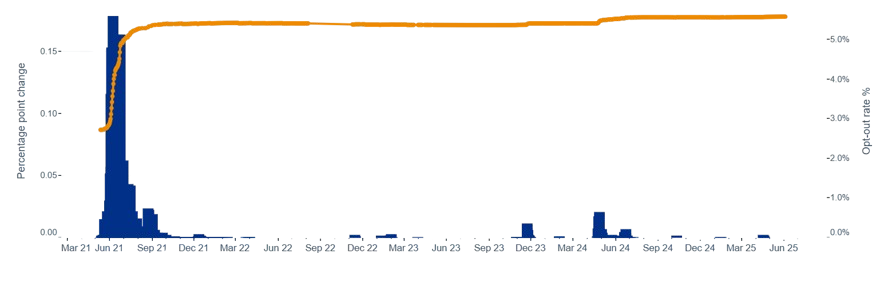
A small number of surgeries report a National Data Opt Out rate of over 50% (one, Wyncroft Surgery in Chelmsford, has a reported opt out rate of 95.6%), which some researchers have suggesed is extremely statistically unlikely and raises questions about whether patients have explicitly opted out themselves.
Frequently asked questions about opt-out in England
What does the National Data Opt-out apply to?
The national data opt-out applies to the use of confidential patient information for planning and research purposes, where exemptions aren’t in place. It applies to work like understanding how health services are working and medical research by pharmaceutical companies, academia, and charities on a local, regional and national level.
The national data opt-out reflects the purposes for using the data, not who or what organisations are using it, or the system the data sits in.
The national data opt-out does not apply where:
-
data is shared for your individual care
-
there is a risk to public health or data is required for monitoring and control of infectious diseases, for example during an epidemic, or food poisoning
-
there is an overriding public interest, for example:
-
reporting of gun wounds in line with General Medical Council guidance
-
there is a legal requirement to share information, for example:
-
investigations by regulators of professionals (eg General Medical Council investigating a registered doctor’s fitness to practice)
-
NHS fraud investigations
-
you have consented to take part in a specific project
-
anonymised (not pseudonymised) data is used.
This website provides further information on where the opt-out doesn’t apply, and where you also may have the ability to make an individual choice.
There are also exemptions made on a case-by-case basis by the Health Research Authority or Secretary of State for Health and Social Care following advice from the Health Research Authority’s Confidentiality Advisory Group, an independent body that provides expert advice on the use of confidential information without consent. It has significant lay representation and other expertise, and thoroughly scrutinises applications. If the group thinks that it is appropriate to use confidential patient information without consent, it’s referred to as Section 251 ‘support’. This is a very significant safeguard in ensuring that this data is used for public benefit in ways that the public would support where there are no alternatives.
The Confidentiality Advisory Group holds a register of all applications that have received approval from the Secretary of State for Health and Social Care, or the Health Research Authority, which can be found on this website. The website also has the minutes from CAG meetings, including a detailed rationale for each application they have advised on. NHS programmes that have Section 251 support can also be found here. The Confidentiality Advisory Group’s remit covers England and Wales.
If you do not set a choice, it will be assumed that you are happy for your confidential patient information to be used for research and planning and you do not need to do anything.
What choice am I offered?
The national data opt-out offers the following choice:
Your confidential patient information can be used for improving health, care and services, including:
planning to improve health and care services
research to find a cure for serious illnesses
Your decision will not affect your individual care and you can change your mind anytime you like.
I allow my confidential patient information to be used for research and planning:
[ ] Yes
[ ] No
What is the impact of choosing to opt out?
Your individual care should not be affected if you opt out using the national data opt-out, but you may be affecting wider research and analysis. This is why UPD feels like it’s important to support people in making informed choices. Research and planning are included together in the national data opt-out; you can’t opt-out of one but not the other. Similarly, you can’t choose specific research or planning activities to opt-out of.
Confidential patient information is used to improve health, care and services across the NHS, for example for monitoring patient safety, planning NHS services like new clinics and understanding differences in health service provision across England. It is also used for research that’s done by:
-
health services
-
universities
-
charities
-
private sector organisations, from large pharmaceutical companies to small med-tech start-ups
What happens if lots of people opt out?
There is no definitive answer to this. We know that opt-outs do affect the quality of some health data analysis, and the more opt-outs, the worse the effects. For example, see this academic paper about how the national data opt-out could have consequences for maternity statistics in England. Sometimes the effects of data opt-outs can be minimised by making assumptions and adjustments, or using information we know from other datasets, but this can reduce accuracy and can lead to more bias (e.g. the results being focused on particular groups in the population rather than all groups). Because opt-outs aren’t randomly spread across the population, groups of people that have more opt-outs are disproportionately affected compared to others (read more about this in our section on how opt out can affect research).
How do opt outs affect research?
Having data about as many people as possible helps to ensure that NHS can make the best, most informed decisions and that researchers are using data that is representative of the population.
Firstly, opt-outs reduce the total number of people we can study for a given question, which can reduce confidence in the results.
Secondly, since levels of opt-out are not consistent across groups, if lots of people from a particular age group, ethnic minority or local area opt-out and this data is used for research, then that group will not be represented in research findings. This can lead to decisions that further impact health inequalities.
To learn more about this, read our guest blog by researchers from the London School of Hygiene & Tropical Medicine about how opt outs impact research.
How do I opt-out using the National Data Opt-Out?
If you wish to opt out using the national data opt-out, there are a few ways to do this for yourself. It is different for children.
Online:
Go to https://your-data-matters.service.nhs.uk/
You will need your name, date of birth, and postcode (registered with your GP surgery) or NHS number. You will also need an email address or phone number registered with an NHS service that you can access so they can send you a security code.
By phone:
Call the helpline on 0300 303 5678
It is open 9am to 5pm Monday to Friday, excluding bank holidays. They can help you use the online service or make or change a choice on your behalf.
By post:
Using this form, which can be posted to:
National Data Opt Out Contact Centre
NHS Digital
HM Government
7 and 8 Wellington Place
Leeds
LS1 4AP
If you want to set a national data opt-out for your children and they are under 13, or where you have a formal proxy to make decisions on behalf of someone else, you can use the same form mentioned above that can be emailed to enquiries@nhsdigital.nhs.uk or posted to the same address as above.
What if I’ve already opted-out using the national data opt-out?
If you have previously opted out of your confidential patient information being shared (e.g. with NHS Digital prior to it merging with NHS England), and want to remain opted out, you don’t need to do anything.
What if I change my mind about opting out?
If you change your mind, you can update your choice by visiting the website: nhs.uk/your-nhs-data-matters, or by calling 0300 330 9412.
What if I’m not sure about whether I have opted-out or not?
If you don’t know if you have opted-out or not, this website will tell you your current choice as part of the process of deciding whether you want to change it.
What other opt-out choices are there?
The opt-out landscape can be confusing and there have been changes over time. There is also, under data protection law, the ability to object to, restrict and delete data processing, but it might not be an ‘absolute’ right. See the ICO’s information on the right to object for more information.
The national data opt-out replaced the ‘Type 2’ opt-out in 2018.
The GP data opt-out, also known as the ‘Type 1’ opt out, means opting out of information leaving your GP surgery. Your confidential patient information would only leave the GP surgery for purposes connected to your individual care and this will continue to apply. If you would like to opt out, or opt in again, you can fill out a form found here and return it to your GP practice. This includes if you’re filling in the form for a family.
The main other opt-outs in the English health system include:
-
Shared Care Record: Shared Care Records are electronic records that bring together different sets of records about your health and care locally. They intend to create a comprehensive and up-to-date record of your health and treatment across the different services that you might use, (rather than your health and care workers sharing relevant information about you with each other on a case by case basis). Some shared care records off a local opt out, and some don’t. More information can be found here.
-
Summary Care Record: Summary Care Record (SCR) is a national database that holds electronic records of important patient information such as current medication, allergies and details of any previous bad reactions to medicines, created from GP medical records. It can be seen and used by authorised staff in other areas of the health and care system involved in the patient’s individual (direct) care. There is also an “Additional Information” section of the SCR, which provides more information such as significant medical history, reason for medication, end of life care information and immunisations. An opt-out is available for those patients that do not want to have an SCR. If you have previously opted out of having an SCR or declined to provide consent to share Additional Information, this preference will continue to be respected and applied. This choice could affect your individual care, and is separate from the national data opt-out. More information is here for the SCR and here for the SCR Additional Information.
-
Cancer registry and congenital and rare disease registries: The National Disease Registration Service includes the National Cancer Registration and Analysis Service (NCRAS) and the National Congenital Anomaly and Rare Disease Registration Services (NCARSRS) are part of NHS England. These are population-based registers that collect information about every cancer patient and patient with congenital (from birth) abnormalities and rare diseases in England. These registries are important to help understand these diseases and provide the best possible care and support. It’s worth noting that even if you choose to opt-out using the national data opt-out, the National Disease Registration Service will still be permitted to collect confidential patient information about you because it has an exemption. However, they won't share this information with others. It is also possible to opt-out of these registries if you prefer.
-
Screening programmes: It is your choice whether or not to have screening. You can opt out of receiving invitations to screening programmes like bowel cancer screening, breast screening and cervical screening. This is something to think through very carefully, because it could mean that early signs of disease may be missed. More information is here.
-
Learning disabilities and autism: Information is collected about people with learning disabilities, autism or both who are getting care in hospitals for their mental health or because they have had behaviour that can be challenging. The purpose of this is so that the NHS can ensure that people are not in hospital if they would be better looked after in the community. This data collection is called “assuring transformation data”. Individuals have the right to object. More information is here.
Why an opt-out rather than an opt-in?
Many different models have been considered. At first glance, gaining informed consent for every use of personal data looks like an ethical approach as it puts patients in complete control. However, this would place a disproportionately high burden on patients – however, this would create an unmanageable amount of work for those who want to object, considering the high volume of projects they would need to opt out of (there can sometimes be around 500 new projects launched each month). From previous research in public dialogues, we’ve found that when people are asked about this, they initially state that they want to be asked for consent for each instance of data use. But talking through what this means in practice often puts them off the idea, as they realise it would require frequent contact and engagement that could feel like a hassle. It is a similar approach that’s been taken for workplace pensions.
Opt-ins also rely on a person making an active choice for their data to be used. This would lead to a much lower proportion of the population’s data being used, because only the most engaged people would take the necessary steps to be included. Everyone else would be automatically opted-out, which would bias datasets and research findings, and worsen health inequalities.
This is why an opt-out system was recommended by the National Data Guardian for health and social care in England and why they are in use elsewhere, too.
However, opt-out systems on their own are not enough. If the healthcare system is asking for people to have trust in the use of patient data, then transparency, accountability, and a strong case for the public and social benefits of using the data are vital. This includes being clear about what choices people have, and how these choices are respected.
We have written about opt-outs before, and this content can be accessed through our news archive.
Why are there opt outs?
There are lots of different views on how health data should be used. Many people are supportive of using it to improve healthcare and research, but feel like they should be asked to give permission first. Others believe their data shouldn’t be used, and this choice should be respected. An opt-out policy enables people to express a choice whilst having a low burden on patients and enabling the highest quality research because the data automatically covers more of the population.
Whether people feel the need for an opt-out policy and to use it depends on many factors, and in particular how people feel about the balance between the risks and the benefits. The more data is used, the more benefits it can bring in terms of contributing to new treatments and finding ways to deal with long waiting lists, for example, but the risk of misuse or data breaches also increases.
For more information on how your data is kept safe, see this page.
What if I want to take part in specific research studies but I don’t want my data used more widely?
Individuals who have set a national data opt-out may still be invited to take part in a research study and can register to be part of research projects. The intention in the National Data Guardian’s Review of Data Security, Consent and Opt-Outs, it was stated that “people should still continue to be able to give their explicit consent separately if they wish, e.g. to be involved in research, as they do now.”
What data systems or private companies does the opt-out affect?
When someone opts out, what they are opting out of is a specific use (or uses) to which their confidential patient could be put (e.g., medical research and service planning). They are not opting out of which system their information can be held in or which specific organisations are using it.
The rules are that people’s health and care data can be stored on any system providing that it:
-
is being used to deliver individual (direct) care to patients and service users
-
is anonymised (so that it’s no longer confidential patient information)
-
is exempt from opt-out due to a legal exemption or government direction
In addition to this, it must also meet the necessary data protection, governance, and security requirements. We recommend that there should always be clear and accessible information available for the public on how health data is handled in all systems.
Many people do not realise that there are private companies that manage data systems and provide analytical services for health and social care organisations, as well as many other parts of the public sector. This can be contentious, which is why transparency is important.
For more information on companies and their access to patient data, please see this page.
What does UPD think about the opt-out policies and the future?
Opt-out policies, like any other policies, are subject to change. This might be because of changes in public opinion and trust, changes in political views, and changes in data infrastructure and processing that alter the balance of risks and benefits.
For example, the National Data Guardian’s Review of Data Security, Consent and Opt-Outs in 2016, mentions that “in future, more person-level data will be required […] because services will increasingly be integrated around an individual”. The Goldacre Review of 2022 stated that the opt-out policy “should be reviewed, but only after a strong national trusted research environment (TRE) has been established for the use of GP data and other commonly used national datasets […] if patient data is only ever stored securely, never directly ‘seen’ by researchers, and used transparently, then there may be fewer circumstances in which it is logical to allow people to opt out; or opt-outs could be reviewed to cover different classes of use, rather than different classes of data flow”.
However, this needs to be thought about carefully. It is a choice that has been given to people, and people’s trust in the NHS or other organisations using their health data is not automatic.
What is certain is that any change to opt-out policy should be discussed in a meaningful way with the public and patients, and it should be reviewed regularly rather than at points of controversy.
UPD have been involved in the topic of choices and opt-outs since the start. As we continue to update our content on the topic, we wanted to ensure our previous articles and blogs are still available. You can find these through the following links:
25/05/2018: Why an opt-out rather than opt-in or consent?
25/05/2018: Is the new national data opt-out just care.data all over again?
25/05/2018: What’s the potential impact of the national data opt-out?
31/07/2018: Guest blog: How the voluntary sector has helped shape the national data opt-out
Where can I find out more?
-
NHS webpages such as NHS national data opt-out programme and nhs.uk/your-nhs-data-matters
-
Further UPD content on why and how patient data is used, and our animations
-
Other third sector organisations, such as https://medconfidential.org/ and https://www.usemydata.org/
-
Medical research charities, such as the Association of Medical Research Charities website